
Hey all,
We’ve all seen them—the patients who don’t look sick, until they suddenly are. Their vitals lull us into false reassurance. Their white count lies. But sometimes, CRP knows first
Case #1: “Cough”
45M, previously well, coming in with 3-day dry cough and fatigue, but looks well
Vitals: T 37.8°C, HR 88, BP 128/78, RR 16, O₂ sat 97% RA
WBC: 9.2
CXR: Normal
CRP: 121 mg/L
He looks great and has normal vitals, normal WBC
What do you do?
Case #2: “Abdominal Pain”
31M, no significant PMHx with a chief complaint of vague right lower quadrant pain
Vitals: T 37.5°C, HR 92, BP 125/82, RR 16
WBC: 10.1
Abdo exam: Soft, minimal tenderness
CRP: 132 mg/L
Normal Vitals, Normal WBC, Exam Underwhelming.
What do you do?
Case #3: “Limping Child”
4F, previously well brought in by her parents because she refuses to bear weight on left leg and decreased range of motion of her hip. She does have a history of a viral cough for the past 3 days
Vitals: T 37.2°C, HR 105, BP 96/60
WBC: 12.4
X-ray hip/femur: Normal
CRP: 89mg/L
She looks well. Maybe just transient synovitis?
What do you do?
Case #4: “Back Pain”
45F, female presents with vague symptoms of low back pain for 2 days. She has a history of drug use but is not clear whether she uses IV drugs.
Vitals: T 37.2°C, HR 85, BP 130/80
WBC: 11.9
L-spine/ Pelvic xrays: Normal
CRP: 98mg/L
Exam: She has no point tenderness, though is quite uncooperative. Ambulates in ED
What do you do?
Answers
Case 1: You nearly discharge him as “viral bronchitis.” But that CRP! Why is it elevated? You push for a chest CT—multifocal pneumonia. Early pneumonia, caught in time. Whew!
Case 2: You aren’t sure he needs imaging. But that CRP seems too high to ignore, so you do a CT. CT confirms perforated appendicitis with small pelvic fluid collection.
Case 3: She looks well, but the labs say otherwise. A joint aspiration is done and confirms septic arthritis. She’s in the OR that night!
Case 4: It seems like non-specific back pain, but you push for an MRI: spinal epidural abscess.
Ok Doc, So, What Exactly Is CRP?
- C-reactive protein (CRP) is an acute-phase reactant produced by the liver in response to inflammation.
So, What Is CRP Telling Me?
- CRP reflects inflammation—especially bacterial.
- It rises quickly (within 6–8 hours) and can peak within 48 hours of an inflammatory stimulus.
- It falls with treatment, so it’s also helpful for monitoring trends in admitted patients.
- It won’t tell you where the problem is—but it tells you there is a problem, often before other tests do.
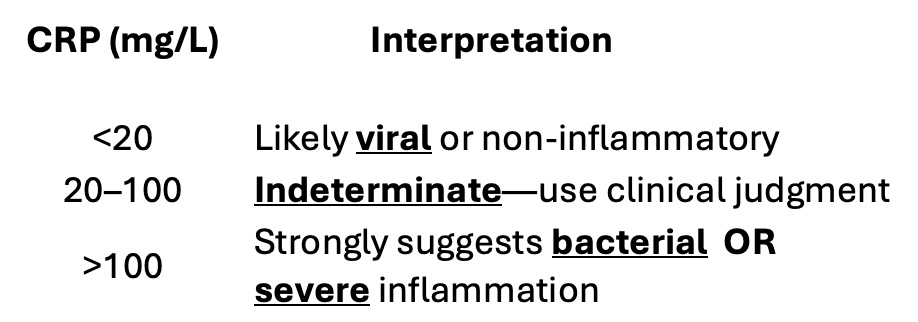
Ok, What Do the Numbers Mean?
When Does CRP Help in the ED?
- When everything looks “okay”
- Normal vitals, reassuring WBC, and no fever don’t rule out bacterial infection—especially in the elderly, immunocompromised, or infants.
- CRP >100 mg/L should trigger a deeper search for source.
- When imaging is negative or borderline
- Negative CXR in early pneumonia?
- Benign abdomen with vague pain?
- Limping child with normal x-ray?
- CRP doesn’t diagnose, but it keeps you from missing the forest for the trees.
- When you’re deciding about discharge
- A CRP <20 mg/L in a well-appearing, afebrile patient can support discharge, especially when your gut says “probably viral.”
- A CRP >100 mg/L with no clear source? You need to dig—or keep them.
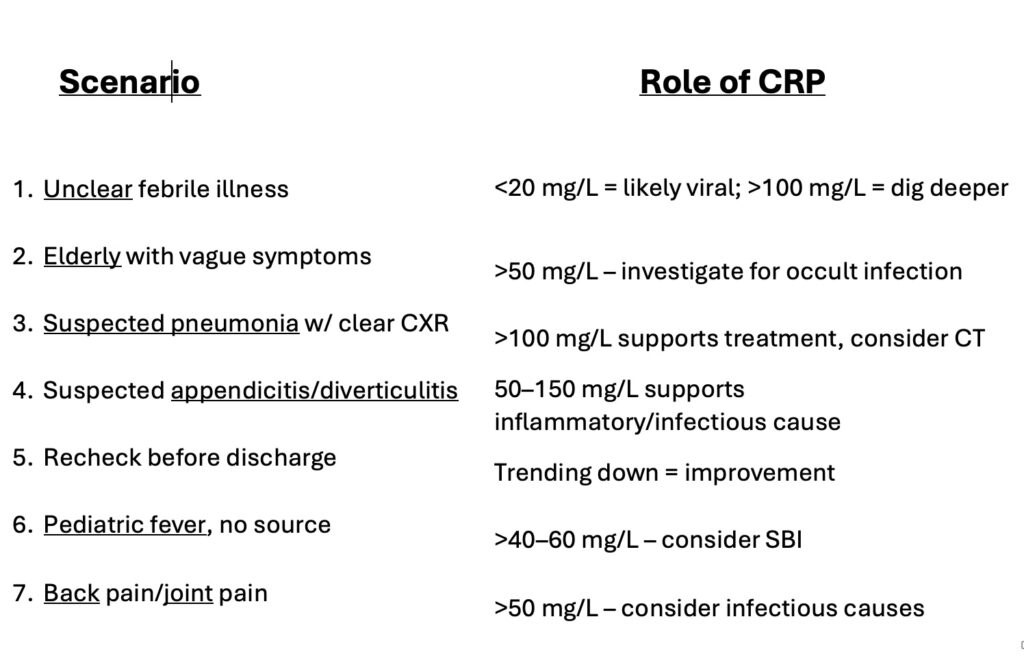
Ok Doc, but how do I Actually Use CRP in Practice
- Undifferentiated Fever
- CRP <20 mg/L: Likely viral, often no antibiotics needed.
- CRP >100 mg/L: Likely bacterial—consider empiric antibiotics and search for source.
- Sepsis Evaluation
- Use CRP alongside lactate, vitals, and WBC to assess severity.
- CRP >200–300 mg/L often signals severe infection.
- Serial CRPs help track response after source control.
- Respiratory Infections
- CRP <20 mg/L: Likely viral—hold antibiotics.
- CRP >100 mg/L: Likely bacterial—even if CXR is borderline.
- CRP 20–100 mg/L: Use clinical judgment and have follow up
- Abdominal Pain & Possible Surgical Abdomen
- Appendicitis: CRP >50 mg/L supports the diagnosis.
- Diverticulitis: High CRP with localized tenderness is suggestive.
- Ischemia or perforation: CRP >150–200 mg/L raises suspicion.
- Pediatric Fever Without Source (≥ 3 months)
- CRP >40–60 mg/L increases concern for serious bacterial infection, especially with abnormal WBC or PCT.
- Back Pain
- Elevated CRP points to an infectious cause
Pitfalls to Avoid
- Don’t delay antibiotics in septic patients just to wait for a CRP.
- CRP can lag—may still be normal if symptoms <6 hours.
- It’s non-specific—can rise in trauma, autoimmune disease, cancer, or surgery.
- Low CRP ≠ Normal. Early disease can still have low CRP.
Summary Table
Take Home Points
- CRP >100 but normal exam? Don’t discharge without knowing why it’s high.
- CRP <20? If everything else looks viral, it probably is.
- In vague cases—especially elderly or pediatric—CRP can be the only early red flag.
- Always interpret CRP in clinical context. It’s not the answer—but it nudges you toward it.
References
Aabenhus, Rune, et al. “Biomarkers as Point-of-Care Tests to Guide Prescribing of Antibiotics in Patients with Acute Respiratory Infections in Primary Care.” Cochrane Database of Systematic Reviews, no. 11, 2024, CD010130.
Froom, Paul, and Margalit Shimoni. “C-Reactive Protein.” Clinical Biochemistry, vol. 49, no. 4–5, Mar. 2016, pp. 291–292.
Pepys, Mark B., and Gideon M. Hirschfield. “C-Reactive Protein: A Critical Update.” The Journal of Clinical Investigation, vol. 111, no. 12, June 2003, pp. 1805–1812.
Sproston, Nicola R., and Jeremy J. Ashworth. “Role of C-Reactive Protein at Sites of Inflammation and Infection.” Frontiers in Immunology, vol. 9, 18 May 2018, p. 754.
Uzzan, Boris, et al. “Procalcitonin and C-Reactive Protein as Prognostic Markers of Sepsis.” Critical Care Medicine, vol. 51, no. 3, 2023, pp. 356–365.
Virk, Ajit, and Jonathan M. W. Chan. “C-Reactive Protein as a Biomarker of Bacterial Infection.” British Journal of Hospital Medicine, vol. 78, no. 7, July 2017, pp. 399–402.

